More than 65 percent of U.S. women aged 40 and over had mammograms between 2013 and 2015, and all of them were protected by a little-known 1992 law called the Mammography Quality Standards Act, or MQSA. Understanding this law is important for radiologists and referring physicians alike, so they can explain it to assure patients that their care meets strict standards of quality. This increases trust between patients and health care providers, ultimately leading to better outcomes.
So what does the MQSA do, exactly? The short answer is that it requires diagnostic imaging providers to produce mammogram images that meet high standards of quality. For a longer, more in-depth answer, we need to look back at the years before Congress passed the law, to a time when breast cancer was "the most compelling health threat to American women," as a 1993 article in the American Journal of Law & Medicine states.
(Though breast cancer rates have been decreasing since 2000, one in 8 women in the U.S. will still develop the illness in 2018. More than 40,000 American women are expected to lose their lives to breast cancer that year.)
In the early 1990s, the American College of Radiology maintained a set of accreditation standards that required monitoring for mammography equipment and staff qualifications. But those guidelines, strict though they were, were entirely voluntary. And as Dr. Charles Smart of the National Cancer Institute toldNewsday in 1991, "Unless mammography is done with quality, there is no use doing it...It isn't enough to get a woman to get a mammogram. It has to be a good mammogram. And it has to be interpreted by someone who is experienced and trained in it."
That wasn't always the case at the time. The Physician Insurers Association of America studied the efficacy of mammograms in the early 1990s and found that 35 percent of women with breast cancer actually had negative results on their mammograms. Another study found that image quality and radiation exposure differed greatly from one diagnostic imaging provider to the next.
By 1992, the effects of this lack of quality had gained the attention of Congress. They acted to pass a bill that would require all diagnostic imaging facilities that conduct mammograms to meet certain standards of quality and to be issued a certificate from the Secretary of Health and Human Services: The Mammography Quality Standards Act of 1992.
What the Mammography Quality Standards Act Requires from Imaging Providers
In order to obtain a certificate, diagnostic imaging providers must meet a distinct set of standards, including, in part:
They must pass a review of their clinical images at least every three years.
These images will comprise a random sample and must be inspected by qualified physicians.
These reviewers must not have a conflict of interest with the sites they inspect.
In addition to the review of images, facilities must pass an annual survey conducted by a medical physicist.
All personnel involved in the preparation and reporting of a mammogram must be certified by the Secretary of Health and Human Services.
A major component of retaining accreditation is the quality of mammogram images themselves. Certified MQSA review physicians carefully inspect a representative range of a mammogram-provider's images. They score these images based on the quality of at least eight criteria:
Correct positioning, such that the chance of missing signs of cancer are reduced.
Adequate compression that avoids conflating motion artifacts and actual tissues.
Perfect exposure; neither underexposed nor overexposed.
There must be enough contrast between light and dark to easily show subtle differences in tissue density.
The image must be sharp, not blurry.
A minimum of visual "noise," or visible artifacts from the imaging process.
No processing artifacts, such as scratches or lint, may be allowed to obscure the structures of the breast.
All images must include identification and other exam details.
The U.S. Food and Drug Administration oversees the MQSA program, and has approved a small group of organizations as "accreditation bodies," or entities that can legally provide the accreditation necessary for conducting mammography procedures. The American College of Radiology is the main accreditation body under the MQSA, but the states of Arkansas, Iowa, and Texas can also provide credentials for facilities located within their borders.
The Costs of Failing to Comply with MQSA
All diagnostic imaging providers that offer mammograms must comply with the quality standards set forth under the MQSA. If they violate any part of the standards, the Secretary of Health and Human Services might issue any of a series of corrective actions, including:
Providing a plan and a timeline for the facility to correct its violation.
The Secretary may order on-site monitoring at the facility's cost.
In egregious cases, the Secretary may order the violator to send notifications to all of their patients, explaining the situation.
For certain violations, the Secretary can issue a fine of up to $10,000.
Ultimately, violating MQSA regulations can shutter a business in two ways. The accrediting body, such as the ACR, could withdraw a facility's accreditation. Or the Secretary of Health and Human Services can revoke the certificate. Owners and operators of facilities that lose their certificates may even be banned from offering mammograms for two years.
How Effective is MQSA at Improving the Quality of Mammograms?
As of the latest report, 8,726 facilities were certified to perform mammograms in the United States, not including VA hospitals. Inspections turned up no violations for 88.5 of these providers.
Patients who are new to mammography may be encouraged to learn that nearly 90 percent of the mammogram providers in the country meet the strict standards of quality required by the MQSA. To learn more about the Mammography Quality Standards Act, see the FDA's website about the program here.
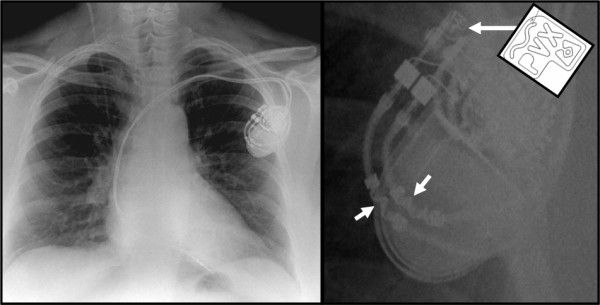
Patients with pacemakers and implantable cardioverter-defibrillators (ICDs) may safely receive magnetic resonance imaging (MRI) testing according to a study from the New England Journal of Medicine. Currently, implanted devices must meet the Food and Drug Administration's criteria to be considered MRI-conditional. The pacemakers and ICDs that do not meet these requirements are considered legacy devices, and the federal government considers them unsafe for MRI scans. However, the new study proves that, with adherence to protocols, patients with legacy devices can safely receive MRI scans.
The study followed over 1500 patients with implanted devices.
The prospective, nonrandomized study followed 875 patients with pacemakers and 634 with ICDs. All patients had implanted devices that were considered legacy devices — that is, they did not meet the requirements of the Centers for Medicare & Medicaid Services (CMS). Researchers from the University of Pennsylvania performed MRIs on the patients only when it was deemed clinically necessary.
The scans were done under strict protocols with physicians on hand to monitor patients. Tachyarrhythmia functions were disabled on the machines and pacing modes were appropriately adjusted on the devices.
“We found MRI examinations to be safe in the setting of legacy cardiac pacemakers or ICD systems, when using a safety protocol,” lead study author and University of Pennsylvania professor Saman Nazarian toldCardiovascular Business. “The scans were safely performed even when performing thoracic or cardiac MRI and with patients that were dependent on cardiac pacing for every heartbeat.”
A previous study from MagnaSafe found similar results for non-thoracic scans.
The MagnaSafe Registry is a multi-center study attempting to determine how safe MRIs are for patients with pacemakers and ICDs. They published findings several years ago that upended the traditional view that MRIs were too dangerous for patients with legacy devices. With similar results to Nazarian's study, MagnaSafe found that there were almost no clinically relevant problems caused by the scan.
This is hugely important because many people with legacy implants are denied MRI scans by Medicare and Medicaid. While doctors may then order computed tomography (CT) scans, MRIs are better at diagnosing certain diseases, particularly in the brain and spinal cord. Nazarian said that if a patient with a legacy device needs an MRI, they should contact a medical center that can safely conduct the scan.
“Many centers across the U.S. are capable of performing safe imaging despite your device,” Nazarian said to Cardiovascular Business. “MRI can be instrumental in providing the right data for appropriate treatment planning in the setting of many neurologic, cardiac and musculoskeletal disorders as well as malignancies.”
The results from the two studies offer compelling evidence that MR technology is safe for those with implanted legacy devices.
According to Robert Russo, a doctor in the MagnaSafe study, more than half of patients with implanted devices will eventually need an MRI. Replacement with an MRI-conditional device is not an option, as the complication risks are too high. Therefore, it's important to determine the safety of MRI scanning for patients with these legacy devices.
The above studies show how MRIs pose minimal risks while bestowing life-saving advantages for those who need scans. The FDA and CMS have not changed their regulations in light of the findings, but the evidence is mounting that they should consider doing so.
Nazarian S et. al. Safety of Magnetic Resonance Imaging in Patients with Cardiac Devices. The New England Journal of Medicine. December 2017;377:2555-2564. doi:10.1056/NEJMoa1604267
A transient ischemic attack (TIA) or commonly referred to as a mini-stroke has traditionally been regarded as a minor and temporary condition, but timely MRIs have proven that these events belong on the same spectrum as strokes. However, because TIAs, by definition, only last a short time, MR imaging must take place as quickly as possible for the fullest yield of useful information.
There is now a consensus that having a TIA increases a person's risk of a stroke.
Approximately one in six people who survive a TIA suffer a stroke within 90 days. Undergoing an MRI as soon as possible after a TIA can detect crucial warning signs that computed tomography (CT) alone cannot see.
Previous consensus guidelines from the American Heart Association (AHA) do not recommend MRI for all TIA patients because of the higher cost. However, mounting evidence suggests that an MRI within 1 to 2 days of a TIA could spot evidence of a stroke that may disappear in time.
MRIs can detect tissue damage even when symptoms are temporary.
The sophisticated imaging technique can detect stroke lesions that may become less apparent quickly. Astudyfrom the journal Stroke followed 263 patients who had suffered a TIA or minor stroke and received a baseline MRI within 24 hours. After 90 days, a follow-up MRI was conducted.
The results of each patient's two MRIs were assessed independently and the results confirm the importance of early scans. Thirty percent of patients with a negative scan at 90 days had a clearly identifiable stroke in the baseline image. Without the early scan, physicians would not know that a stroke had occurred in this large group of patients.
In spite of this evidence, some physicians settle for a less-precise CT scan. A recentstudyfrom Neurology found that just 40 percent of patients with TIA or minor stroke had an MRI performed within 48 hours.
New guidelines offer options for those at high-risk of stroke.
The AHA and American Stroke Association have published new consensus guidelines for preventing strokes in patients with a history of strokes or TIA. Reducing hypertension and statin therapy remain at the top of the list. Increasing physical activity, reducing sodium intake, and following a Mediterranean-style diet (as opposed to a low-fat diet) are recommended. Other practices, such as sleep assessments and anti-platelet therapy immediately following a TIA may be considered.
For patients with a history of stroke or TIA, the average annual rate of future stroke is at an all-time low. That's great news, but a more nuanced understanding of TIAs and timely MRI of those who suffer them could yield even more impressive results.
References:
AHA and ASA Release Guideline for Prevention of Future Stroke in Patients with Stroke or TIA. American Family Physician. January 2015;91(2):136-137. Available from: https://www.aafp.org/afp/2015/0115/p136.html
Chaturvedi S et al. Have clinicians adopted the use of brain MRI for patients with TIA and minor stroke? Neurology. January 2017;88(3):237-244. doi:10.1212/WNL.0000000000003503
Moreau F et al. Early Magnetic Resonance Imaging in Transient Ischemic Attack and Minor Stroke: Do it or Lose it. Stroke. March 2013;44(3)671-674. doi:10.1161/STROKEAHA.111.680033
A first-time MRI procedure can make patients nervous, even to the point of ending the scan. That can lead to higher costs for imaging centers, and even affect patient outcomes if the anxiety interferes with the quality of the radiology report. Research shows one simple way to help nervous patients get through their scans without interruption: Communication.
A 2015 study in the journal Magnetic Resonance Imaging tested an intervention in which imaging staff explained the MRI process to one group of patients. They took blood samples during the scans, later testing them for the stress hormones prolactin and cortisol. Additionally, they took both the experimental and control groups through the 40-questions State-Trait Anxiety Inventory to measure patient nervousness.
The patients who had the intervention in which staff verbally shared information about the scan showed a 6-percent drop in cortisol after the scan. The control group's cortisol levels increased by 18 percent. The authors of the study conclude that "MRI anxiety can be reduced by information and communication. This combined method is shown to be effective and should be used during daily radiology routine."
So what can physicians do to prepare their patients for a first MRI scan in advance? It's never too early to start educating patients about what they can expect during a health procedure. And the MRI process can be boiled down into 10, easy-to-grasp steps. Share these steps with patients to help limit anxiety during an MRI scan:
First, radiology staff will walk the patient through a detailed screening process. Because of the strong magnetic field generated during an MRI, patients must report any medical implants or metal particles in their bodies. These may preclude the use of MRI imaging.
Once the patient clears the screening, staff will lead them into the MRI suite. Some imaging facilities offer hospital robes, to ensure there's no metal in the patient's clothing. Others allow patients to wear their own metal-free clothes, such as sweat pants and a T-shirt. The technologist will proceed to position the patient on the table; most commonly, patients lie on their backs. If the scan requires an additional radiofrequency coil, the technologist will place that on the patient's body at this time.
The patient enters the bore. Meanwhile, technologists cycle through a list of pre-programmed settings called "protocols." They'll choose the protocol that corresponds with the body part they are imaging; this will tell the MRI machine which angles, targets, and pulse sequences to use in this particular procedure.
Before the scan proper begins, technologists run a "scout" or "localizer" scan. This is a low-quality image, and it won't be used in reporting. However, localizer scans obtain visual and placement information that the computer will used to plan the angles of its imaging later in the process.
Parallel imaging is a process designed to speed up scan time. It collects less raw data during the scan, and patches missing information using special algorithms to generate the final image. Parallel imaging requires specifically calibrated coils, and may call for a calibration scan at this point.
One of the great strengths of MRI scans is that they create 3D images that can be viewed from any angle. The next step is to program in the angle of images for the radiologist. Technologists can change the "thickness" of the image at this point, as well.
Before the scanner can begin collecting valuable images, it must calibrate all systems through the use of a prescan. This shouldn't take much more than 10 or 20 seconds.
It is only at this relatively late stage in the process that the technologist actually runs the scan. They will make necessary adjustments and continue scanning according to the chosen protocol. In the end, they'll have clear, accurate images that radiologists will use in their reporting.
Some types of images require extra work in post-production, but this can be done after the patient has left the MRI suite.
Scanning complete, the technologist pulls the patient from the bore. Different types of scans take varying lengths of time, but most range between 20 and 60 minutes.
When patients understand more about their medical procedures, and know what to expect, they're less likely to experience significant anxiety. That's both a value in itself — as patient-centered caregivers, staff at Precise Imaging works to keep patients comfortable, both physically and emotionally — and an element of better diagnoses, which lead to better patient outcomes.
To learn more about an MRI procedure from Precise Imaging, or to refer a patient, call us at 800-558-2223.
References:
Deshmane A, Gulani V, Griswold MA, Seiberlich N. Parallel MR imaging. Journal of Magnetic Resonance Imaging: JMRI. 2012;36(1):55-72. doi:10.1002/jmri.23639
Tazegul G, Etcioglu E, Yildiz F, Tuney D. Can MRI related patient anxiety be prevented? Magnetic Resonance Imaging. 2015;33(1):180-3. doi:10.1016/j.mri.2014.08.024
Independent imaging centers are moving to the forefront of diagnostic care in the United States. Recently, at least one major health insurer dropped coverage for CT and MRI scans at hospital radiology facilities. The insurance company will only pay for these scans when patients visit providers who specialize in diagnostic imaging, and imaging alone.
How will this change the conversation between referring physicians and their patients? In order to explain the changes — why insurers would make a rule like this, and why it's not at all a bad change for patient care — physicians need only look at two key metrics of today's health care system: price and quality.
The Price Difference Between Hospitals and Independent Imaging Centers
When an insurance company makes a move like this, it's a clear indication that there's a wide price differential that's not necessarily associated with a difference in quality of care. Research from the Healthcare Financial Management Association — a professional organization for people who work on the financial side of the health care industry — shows that prices at hospitals are, in fact, dramatically higher than those at the average free-standing imaging provider. Among other differences, the HFMA found:
MRI scans cost an average of 70 percent more at hospitals than at independent imaging centers.
When those MRI scans covered the head and/or neck, they were an average of 80 percent more expensive in hospital-owned facilities.
The differences were even more stark for CT scans. Imaging of the body using CT cost 135 percent more at hospitals.
For CT scans of the head and/or neck, patients paid an average of 149 percent more at hospitals than at free-standing imaging facilities.
This research was published in 2017, though most of its data came from 2014. Either way, price gaps remains.
Measuring the Quality of Diagnostic Imaging Providers
Patients are used to associating higher prices with better service. In health care, however, quality and cost are independent of one another. The United States has the most expensive health care in the world.
In 2014, U.S. health care spending per capita was $9,237. That year the United Kingdom spent $3,749 per person while Japan's figure stood at $3,816. Still, among the 12 wealthiest industrialized nations — including Japan and the UK — the United States lands dead last in terms of life expectancy.
Clearly, spending more does not buy better care in this country. In fact, independent imaging centers offer measures of quality, in terms of better patient experience, that most hospitals cannot boast. At Precise Imaging, these include:
Evening and weekend hours to work around the patient's schedule, not the other way around.
Excellent, board-certified radiologists and technicians, often the same ones hospitals use, at a drastically reduced cost.
Quick reporting with HIPAA-compliant online sharing with referring physicians. Most doctors are reading radiology reports within 24 hours of the scan.
Same-day scheduling.
Transparent pricing.
There have been plenty of good reasons to refer patients to a free-standing imaging facility for years. Now that insurers are refusing to support the arbitrary and inflated costs that hospitals charge, more and more patients will be able to experience the care that Precise Imaging provides.
Personal injury attorneys have relied on MRI scans to bolster their clients' claims for years, but the role of this crucial technology may soon grow dramatically. As a diagnostic imaging modality, MRI is ideal for recording soft tissue injuries, including disc protrusions and herniations and muscle tears. But even perfect documentation of these injuries doesn't necessarily prove a devastating type of affliction that's all too common, and often difficult to demonstrate: chronic pain.
Pain is a subjective sensation. One person's agony might be another's slight discomfort, and defense attorneys have a history of leaning on this subjectivity to reduce damages. Meanwhile, though, patients' lives can be destroyed; ravaged by pain, they might not be able to work, or even perform daily tasks of living. A fair settlement might be the only thing that stands between them and utter destitution.
But how can an MRI scan document pain? Neuroscientists say they're right on the verge of an answer.
Using MRI Technology to Track Pain's Pathways in the Brain
A specialized type of MRI scan, functional magnetic resonance imaging, or fMRI, measures blood flow within the brain. When a certain region of the brain activates, cerebral blood flow in that area increases. The fMRI tracks these changes.
Brain mapping allows neuroscientists to associated certain areas of the human brain with general functional experiences within the thinker — including, perhaps, the thinker's experience of pain. If an attorney could demonstrate that a client's brain activity is consistent with chronic pain, that could be enough to sway the judge. However, we're not quite ready to break out the fMRI scans in tomorrow's personal injury case.
Hurdles in the Use of fMRI Scans for Personal Injury Cases
Neuroscientists are still debating the reliability of fMRI to demonstrate chronic pain. Most of the studies involving pain and brain mapping have been conducted on acute pain, not the chronic variety. Some scientists argue that patients could "cheat" the scan, imagining a greater-than-baseline intensity of pain.
The science behind demonstrating pain with fMRI scans isn't quite up to courtroom standards yet, but it's close, and it's getting closer. With every new study on the subject, fMRI technology inches toward a future in which pain is as visible as a broken arm in an X-ray.
Meanwhile, standard MRI scans continue to be an important element in many personal injury cases. This technology has changed the way personal injury law functions, and it appears it will continue to do so in a broader range of cases soon.
Patients and referring physicians increasingly enjoy the benefits of digital access to radiology reports, but the online environment raises new concerns about HIPAA compliance.
It is, of course, entirely appropriate for doctors to be concerned about patient privacy online. In May of 2017, at least 7,000 medical records were leaked at a New York City hospital. In November of that year, hackers took hostage the protected health information of 7,000 patients at a Massachusetts sports medicine provider, demanding a ransom with the threat of releasing the data. The following month, news broke that an ex-employee of a San Antonio mental health provider left the job with more than 28,000 patient records downloaded to a personal computer.
Data breaches happen, and when they do, health care providers could find themselves in violation of HIPAA. So how can physicians be sure that their radiology providers are adequately protecting their practices and their patients?
Here, we describe some of the ways that the Precise Imaging web portal does it. By following these recommended protocols, our IT systems keep out intruders, ensuring compliance with HIPAA to keep protected patient information safe and secure. First, though, we'll take a look at the letter of the law itself. What exactly does it mean for an online data-sharing system to be "HIPAA-compliant?"
The Health Insurance Portability and Accountability Act of 1996 and Patient Privacy
According to the HIPAA Security Rule, which governs the storage and transmission of electronic protected health information (EPHI), requires covered health care providers to meet four major goals:
The provider must keep EPHI in their possession — whether they create the information, hold it, or simply pass it along — completely private and confidential. It cannot become available to any non-approved parties.
Within reason it is the provider's responsibility to anticipate potential threats to secure information. If they identify a threat, they must act to protect EPHI from it.
Similarly, providers have a duty to shield EPHI within their control from "unauthorized uses or disclosures."
Finally, these requirements extend from top administrators to the very bottom of the pay scale. Every health care provider must make sure that all employees comply with the above rules.
Note that the Security Rule does not dictate specific technical steps companies must take to keep EPHI safe and secure. These things are up to the providers. And the entities covered under HIPAA have strong incentives for investing in ironclad digital protections for their patients' health information: They can face fines of up to $50,000 per compromised health record, with an annual maximum limit of $1.5 million.
But there's an even more important reason why responsible health care providers invest heavily in protecting patient information. Organizations that devote themselves to patient-centered care don't just treat a single injury or illness and forget their patients. They concern themselves with every aspect of the patient experience, from physical and emotional comfort to mental well-being between visits, as much that's possible. Finding out that your personal information has been leaked is a stressful experience, and no self-respecting health care provider wants to bring anxiety into a patient's life. In short, we invest heavily in privacy because that's what's best for the patient.
HIPAA Compliance in the Radiology Web Portal
Precise Imaging offers a series of user-specific web portals, for patients, referring physicians, and even personal injury attorneys who may need access to diagnostic images to win a case. Each of these web portals provides best-in-class security features, clearing HIPAA requirements and protecting our users' priceless data.
The following is far from an exhaustive list of the security tools that protect radiology reports and other EPHI within Precise Imaging web portals. But it should make clear that these systems are robustly protected from data loss that could put patient information at risk. Here are a few of the tools that our IT systems have in place to protect EPHI and comply fully with HIPAA requirements:
All transfers of EPHI through the Precise Imaging web portals are fully protected by SSL/TLS encryption.Transport Layer Security (TLS) is the industry standard for protecting data in transit from clients to servers and back again. This is an updated version of Secure Sockets Layer encryption (SSL), but we refer to the technology as "SSL/TLS" because people still tend to use the terms interchangeably. In fact, TLS is more advanced than SSL encryption, and that's what our web portals use to encrypt data in transit.
Data remains secure even in a computer's local cache through AES, the Advanced Encryption Standard. This block cipher algorithm is one of only two encryption tools used by the U.S. government, and it remains a powerful lock on data. To further protect data within the local cache, these web portals purge the cache of EPHI after each session. That is, after the user logs out, there's no patient information stored locally at all.
Site administrators set strict user identifiers. Each user must have a unique login ID and password, and our systems don't allow weak passwords. We may even ask for periodic password replacements; all of these systems are designed to keep EPHI as secure as possible.
Audit trail tools track each user's activities (without storing EPHI). If, somehow, an unauthorized user gained access to one of our web portals, integrated reporting tools would flag any suspicious activity.
After a period of inactivity, sessions will logout automatically. This reduces the chances of an unauthorized viewer gaining access to EPHI when users simply forget to log off.
The servers that Precise Imaging web portals use are configured specifically to comply with HIPAA. When it comes to patient data, we don't take chance. Server rooms that host patient data are even equipped with comprehensive physical security, greatly reducing the risk of intrusion.
There's no reason that compliance with HIPAA should reduce the web-based functionality that so many radiologists, referring physicians, and patients rely on to create better health outcomes. At Precise Imaging, we follow advanced security protocols to protect patient information. We're able to share online radiology reports with full HIPAA compliance, which tends to reassure even the most security-conscious referring physician we work with.
Gefen R, Bruno M, Abunedeh H. Online portals: Gateway to patient-centered radiology. American Journal of Roentgenology. 2017 209:5, 987-991. doi.org/10.2214/AJR.17.18291
Lee, CI, Langlotz CP, Elmore JG. Implications of Direct Patient Online Access to Radiology Reports Through Patient Web Portals. Journal of the American College of Radiology. 2016 13:12PB, 1608-1614. doi.org/10.1016/j.jacr.2016.09.007
Radiologists and referring physicians need dependable, clear communication to collaborate on accurate diagnoses for their patients. When that communication is lacking, the risk of errors can quickly compound.
Annette Johnson, MD, MS, describes a particularly worrisome case on the Agency for Healthcare Research and Quality website. This is an example of what can go wrong when physicians and radiologists don't have quick, easy-to-use access to one another.
Radiology Report Transmission Errors: An Alarming Story
A 62-year-old man was admitted to the hospital with swelling in his abdomen and legs, Johnson reports. His right leg was slightly more swollen than the left, and the attending physician was concerned that he might have a deep vein thrombosis (DVT). The physician ordered an ultrasound to check for evidence of a blood clot.
The imaging procedure didn't show any signs of DVT. The radiologist called the primary care team and told them this verbally after dictating the report, so the team continued to treat the man with the understanding that he did not have a DVT. All was well up to this point.
The problem occurred when the night team rotated in. As the radiologist verbally dictated the report, it turns out, the dictation system clicked just as it recorded the words "no DVT is seen" — obscuring the word "no." As a result, the hospital's voice recognition software recorded the phrase "DVT is seen." That's the statement that made it into the truncated radiology report, which the night resident read when beginning the shift.
This confusion eventually led to two unnecessary surgeries: One to place a filter in a blood vessel leading to the lung, to block the (nonexistent) blood clot; and the other to remove the filter after someone finally tracked down the reporting radiologist and learned about the mistake. The good news is that there were no complications, and the patient emerged from the surgeries no worse for wear.
Improving Communication Between Radiologists and Referring Physicians
So where did the care team go wrong in this case? Let's break the issues down into two categories: technology and procedure.
There were two clear technology issues in this case: First, a microphone that clicks when activated, and second, the voice recording software's inability to understand the word "no" beneath the click.
But the case also illustrates the simplest way around reporting errors. Remember that when the patient was first admitted, the reporting radiologist spoke directly to the primary care team. That sort of one-on-one interaction is ideal.
At Precise Imaging, we offer a physician's web portal that allows real-time sharing, analysis, and annotation of diagnostic images. This provides yet another way for physicians and radiologists to collaborate directly, no matter where they are.
As for procedural issues, Johnson points out that dictation using VRS is more error-prone than using human transcriptionists. Of course, her report dates back to 2011, and voice recognition systems have improved since her estimation.
The team also missed the opportunity to provide all physicians involved in the patient's care with access to more information — while the truncated radiology report might have read "DVT is seen," with access to images, annotations, and detailed analysis, the night resident might not have proceeded under the assumption that a blood clot was present. Again, comprehensive image-sharing web portals for physicians offer greater communication between radiologists and physicians.
Physician web portals aren't the only innovation that can improve information-sharing between all members of a medical care team. You also need experienced, board-certified radiologists who work onsite in the U.S. to read diagnostic images, such as those at Precise Imaging.
All of our radiologists are devoted to patient care, and that means excellent communication with doctors, every time. Radiologists and referring physicians can work together to improve patient outcomes — but only if they commit to quality communication.
Breast MRI is not a first-line breast cancer screening tool for most women. The American Cancer Society recommends annual MRI screening only for women with a lifetime risk of breast cancer that's greater than 20-25 percent, and only as an adjunct to mammography. The problem is that MR images are too clear, leading to too many false positives, the ACS explains.
"While the high rate of biopsies and further investigations is acceptable in women with a high risk of breast cancer, the number of such investigations in women at lower risk will be much higher than would be appropriate, leading to the need to counsel women in lower risk categories that MRI screening is not advisable and that the harms are believed to outweigh the benefits," wrote researchers for the American Cancer Society Breast Cancer Advisory Group in the ACS guidelines in 2007.
However, a study published in the May 2017 issue of the journal Radiology suggests that it could be time to rethink these recommendations. Researchers from the University of Aachen studied 2120 women, aged 40 to 70, with lifetime breast cancer risk factors of less than 15 percent. The women received screening via MRI, ultrasound, and mammography between 2005 and 2013.
Of the 60 cancers discovered in the study, 59 were observed using MRI scans. None were uncovered by ultrasound or mammography alone. Meanwhile, the positive predictive value of the MRI screening was high, hinting that concerns over false positives may be exaggerated given current MR technology and advances in radiology practice.
"In women at average risk for breast cancer, MR imaging screening improves early diagnosis of prognostically relevant breast cancer," the authors concluded.
Other Factors Limiting the Use of Breast MRI Screening
Even if further studies show that false positives are no longer as prevalent in MRI breast screening as they once were, other barriers continue to limit patient access to the procedure.
There are two major reasons physicians don't order more breast screening via MRI, reportsRadiology Today magazine: Insurance companies won't cover breast MRI for women unless they show high risk, citing excessive costs for the procedure; and there simply aren't enough MRI providers across the nation.
These are concerns that patients and physicians in many parts of California, Nevada, and Arizona needn't worry about. Precise Imaging operates a growing network of more than 70 free-standing imaging centers in communities across these states — with more on the way.
Precise Imaging Expands Access to Breast MRI Scans
By providing access to MRI scans within many communities, Precise Imaging allows patients to schedule appointments when and where they please. This greatly expands the total MRI capacity in areas where Precise Imaging operates.
As for the issue of cost, Precise Imaging provides a streamlined, flexible billing system, allowing patients to pay through as many avenues as possible. That includes Medicaid/Medicare, PPO insurance, personal injury liens, letters of protection, and low cash prices.
And because Precise Imaging providers aren't attached to a broader hospital system, they don't have to balloon prices to cover high-loss areas, such as emergency services. Together, these factors allow Precise Imaging to offer more diagnostic imaging procedures — including breast MRI — to more patients at a lower cost.
Some day soon, breast MRI might becomes a standard screening procedure for all women, with life-saving results.
References:
Kanal K, Butler P, Sengupta D, Bhargavan-Chatfield M, Coombs L, Morin R. U.S. Diagnostic Reference Levels and Achievable Doses for 10 Adult CT Examinations. Radiology. 2017 284:1, 120-133. doi:10.1148/radiol.2017161911
Saslow D, Boetes C, Burke W, et al. for the American Cancer Society Breast Cancer Advisory Group. American Cancer Society Guidelines for Breast Screening with MRI as an Adjunct to Mammography. CA: A Cancer Journal for Clinicians. 2007 57: 75–89. doi:10.3322/canjclin.57.2.75
Precise Imaging to Open New Anaheim Location, Expanding Availability of Patient-Centered Diagnostic Care with Unparalleled Access for Physicians
November 10, 2017 — Anaheim, California — Precise Imaging, a private corporation owned by Jaklin Benji, Matt Benji and Mike Rashidi, will open a new facility at 3174 West Lincoln Ave., in Southwest Anaheim, on the 13th day of November 2017. As a leading independent provider of diagnostic imaging services across California, Nevada, and Arizona this latest location will feature a state-of-the-art open MRI scanner. The opening of an Anaheim location will create even more flexibility for those in need of imaging services while expanding access for referring physicians and their patients.
"Access to quality care is our highest priority," said Danny Rackow, director of technology and operations at Precise Imaging. "The new Anaheim location gives doctors and patients yet another quality source for MRI procedures while bringing the benefits of an open MRI to a whole new community."
The Anaheim location adds to Precise Imaging's growing network of over 100 locations, many of which offer evening and weekend hours, same-day referrals, and 24-hour turnaround on radiology reports—even less for STAT cases.
Patient-Centered Care with Physician-Preferred Workflow
In keeping with Precise Imaging's mission to build dependable relationships with referring physicians in every medical specialty, the new location will offer a powerful suite of digital resources for health care providers. Physicians can make referrals at any time through a free online form. Following the procedure, they can view radiology reports and images 24 hours a day through a simple, HIPAA-compliant web portal. Experienced IT staff is available at every hour of the day and night to assist physicians with all digital tools.
"Doctors should be able to focus on care and not get bogged down on the simplest interactions such as scheduling, availability and ease of use with a provider," Mike Rashidi said. "We built our physician access tools to make the entire process hassle-free, from referral to reporting to interacting with insurance providers, because we want what the doctors want: better health outcomes for patients."
Precise Imaging has a proven track record of patient satisfaction, and the new location will continue this tradition. The inclusion of a comfortable open MRI scanner in the latest facility is just one example of the compassionate care that sets Precise Imaging apart. Friendly, experienced staff and board-certified radiologists take the time to provide support for the whole patient—body and mind—and that can lead to better, more actionable reports.
Continued Partnerships with Personal Injury and Workers' Compensation Attorneys
*Legal professionals who serve clients in Anaheim will benefit from the establishment of the new Precise Imaging location. The company has a long history working with injured clients, and has developed a streamlined and efficient work flow that can provide case-winning medical evidence right on schedule.
*Physicians can refer a client online with the click of a button and reach out for support any time through a dedicated web portal. All Precise Imaging locations accept personal injury liens, letters of protection, and workers' compensation liens.
"We've helped thousands of attorneys seek justice for their clients, and that mission continues with our new facility," says Matt Benji.
To learn more about Precise Imaging's new location, or to schedule an appointment anywhere in the network, call 800-558-2223.
About Precise Imaging
Precise Imaging is a leading provider of MRI, X-ray, PET, and other diagnostic services with locations across California, Arizona, and Nevada. The company offers industry-leading support for physicians and attorneys with best-in-class patient care. Flexible billing options include Medicaid/Medicare, PPO insurance, personal injury liens, cash prices, and more. To learn more about Precise Imaging, please visit www.precisemri.com.