Will Artificial Intelligence Replace Radiologists One Day?
Artificial intelligence (AI) has undergone dramatic growth in recent years; its effects can be seen in virtually every field, from oil drilling to games of chess. Deep learning, a method which teaches computers to recognize objects within pictures, has significant potential impact on the medical imaging field.
That’s why some AI researchers say the technology could spell the end of human radiologists. Computers, they say, would be able to quickly, cheaply, and accurately perform the same job functions. While the power of AI cannot be denied, it seems premature to make assumptions about the important role trained human radiologists play in the contemporary health care industry. Artificial intelligence will almost certainly help radiologists do their jobs; we just doubt it can replace them entirely.
Radiologists may certainly be worried about the future of their profession, but any concern would be premature at this point. In fact, the adaptation of AI into imaging technology has great potential for increased productivity among radiologists and increased profitability for those institutions housing them. There are several current and future avenues in which AI may prove a useful augmentation to radiologists, as well as certain restrictions which ensure radiologists will continue to have gainful employment well into the future.
How AI Can Improve Radiology as the Tool of Human Radiologists
The first way in which AI may serve radiologists is in a quicker diagnosis of certain types of fractures and cancers. This would free the radiologist for more difficult-to-detect cases that could not be handled by current machine learning technology. In many cases, AI could also confirm a diagnosis that may have otherwise been in doubt, providing clinical decision support. The increased usage of deep learning in imaging also would allow the radiologist to spend more time focusing on the patient and their treatment plan, potentially creating greater job satisfaction for that individual.
A second major reason for the medical field to embrace AI is the potential for increased demand in imaging procedures. In countless cases throughout history, increased automation meant greater efficiency, which in turn brought the price of the given product down. Often throughout history, increased automation brought about fears of workers losing their jobs; however, the lower prices usually resulted in such a significant uptick in consumer demand that more jobs were created than lost. The same potential exists for the relationship between AI and radiologists.
Third, many conflate the type of AI learning being applied to radiology with the AI seen in science fiction movies. The deep learning being applied in to diagnose fractures or occurrences of cancer is an extremely focused technology used for that purpose and that purpose only. The AI is not suggesting a treatment pattern, or consoling a patient who has received devastating news. AI is only reading an object in a picture, albeit to a highly accurate degree in some cases.
Why Human Radiologists Will Always Be Part of Diagnostic Imaging
No machine will ever be able to replace the empathy that medical providers develop throughout their careers. There’s no substitute for a warm hug, a meaningful conversation, or time spent with a trusted physician.
Artificial intelligence has the potential to greatly alter the field of radiology in many ways that generate a positive impact for all those involved, from the patient to the radiologist to the medical institution. Imaging specialists need not worry about job loss at the hands of a faceless algorithm. Instead, opportunities to increase patient well-being and diagnoses accuracy should be adopted whenever possible.
Traumatic brain injury (TBI) can be one of the most devastating results of an at-fault accident, in a car, on the job, or even just walking down the sidewalk. The sheer volume of human systems that the brain controls — all of them, essentially — leads to an extraordinarily diverse set of symptoms in cases of TBI. Convincing judges and jurors that these disparate symptoms can all be traced back to a preventable injury is not always easy.
The irony here is that a moderate or severe TBI can lead to challenges that most deserve restitution. Some brain injuries are so severe that they deprive the victim of the ability to work. Others might even prevent a patient from participating in the tasks of daily living necessary for independence. If a client in a TBI-related personal-injury case is to be made whole, settlements may have to provide for them for the rest of their lives.
This combination of high stakes and soft proofs makes it imperative that attorneys in such cases understand diagnostic imaging. After all, while a defense team may be able to convince the judge that behavior changes are unrelated to an accident, it is hard to argue with an image of a damaged brain.
Here are a few things that personal injury lawyers should know about diagnostic imaging as it relates to TBI:
Different modalities excel at documenting different types of injuries. Radiologists are likely to use standard diagnostic tests like CT and MRI scans to diagnose TBI. They might order X-ray scans, but only in cases of suspected damage to the skull; X-ray images do not differentiate between soft tissues. Doctors might even prescribe advanced imaging techniques, such as perfusion CT, diffusion tensor imaging (DTI), or magnetoencephalography, a form of fMRI.
CT scans without contrast are the primary modality used to identify most primary, acute injuries. A TBI is not a single injury, but a cluster of related events. Doctors divide TBI into primary and secondary injuries. The first occurs at the moment of impact, causing a chain-reaction of events within the brain that often lead to further damage: secondary injuries. This is why doctors typically prescribe ongoing diagnostic imaging for TBI patients.
While advanced imaging modalities including brain-function tests like PET scans and functional MRI may identify secondary injuries, the first-line test for diagnosing primary TBI is the noncontrast CT scan. This is the fastest way to accurately expose bleeding that requires immediate surgery.
Doctors use MRI scans to identify certain types of TBIs that do not always show on a CT scan. While doctors typically order CT scans first, there are some types of TBI that require MRI for identification. When a primary TBI does not result in intracranial bleeding, MRI scans are often the better choice. Injuries that the MRI identifies better than CT scans include brain bruising and traumatic axonal injury (TAI), shear-strain damage to white matter caused by the brain's rapid acceleration within the skull.
As in any case involving diagnostic images, attorneys should engage expert witnesses such as neurologists or radiologists to explain what's going on in the pictures. This is particularly important in brain-function scans, such as fMRI and PET scans, which are often inscrutable for untrained viewers.
The good news for attorneys new to TBI cases and the diagnostic interventions that document them is that expert help is available. This brings us to our next point.
Expert Assistance for Personal Injury Cases Representing Victims of TBI
Personal injury lawyers and their clients deserve the chance to focus entirely on a TBI case. That can't happen when they're navigating complex scheduling systems at large hospitals or arguing with insurance companies. That's why Precise MRI always strives to provide for attorneys and their clients with what they need, when they need it.
Precise MRI offers quick turnarounds on radiology reports, with same-day scans and results within 24 hours. We provide more than 70 imaging centers in California, Arizona, and Nevada for convenient, close-to-home access for patients. Our friendly scheduling staff will find an appointment that works for your client, even on weekends and evenings.
Attorneys themselves have their client's crucial information at their fingertips thanks to an online portal designed for legal professionals. It's available 24/7, and so is IT service, ensuring that patients and their lawyers can access medical data at their own convenience.
We accept personal injury liens — and even offer a free, downloadable lien form for immediate access — and attorney letters of protection for personal injury. Our teams of fully certified medical professionals have long-term experience working with attorneys on all sorts of personal injury cases, including those involving TBI. Even more important, they're devoted to a patient-based model of care, and work hard to ensure quality, comfort, and convenience for all.
To learn more about attorney resources from Precise Imaging, or to schedule a CT or MRI scan for a client, call us today at 800-558-2223.
References:
Hill CS, Coleman MP, Menon DK. Traumatic Axonal Injury: Mechanisms and Translational Opportunities. Trends in Neurosciences. 2016;39(5):311-324. doi:10.1016/j.tins.2016.03.002.
Kim JJ, Gean AD. Imaging for the Diagnosis and Management of Traumatic Brain Injury. Neurotherapeutics. 2011;8(1):39-53. doi:10.1007/s13311-010-0003-3.
There are currently 5.7 million people living with Alzheimer's disease (AD) in the United States, and this number is projected to reach 14 million by the year 2020. As of 2018, AD was the fifth-leading cause of death of seniors, taking more lives than breast or prostate cancer combined. With such staggering and ever-increasing numbers, the need for early detection and treatment has reached a crisis point.
But understanding AD hasn’t been easy. Researchers have struggled to identify the true cause of this disease, develop a standard treatment plan, or find a cure. While an AD diagnosis may seem dire, early detection of the disease can help identify how the disease progresses, which in turn can help to create a treatment option.
New Research on AD Biomarkers and How to Detect Them
Recent research has shown a connection between changes in the brain’s anatomy and biomarkers known to appear at the early signs of AD. These biomarkers occur before any sign of cognitive problems, meaning these markers could possibly lead to a new, non-invasive AD screening test. Researchers have already discovered that the build up of amyloid-Beta and tau proteins on the brain, as well as a loss of volume in the hippocampus, are early signs of AD.
To further examine any links between these two phenomena, researchers from McGill University and McGill-affiliated health institutes studied 88 AD at-risk individuals with no signs of any cognitive decline from the disease. The subjects were given MRI scans to check brain volume, and also had cerebrospinal fluid samples taken to test levels of amyloid-Beta and tau proteins.
The researchers found that high levels of both amyloid-Beta and tau proteins were associated with loss of hippocampus volume, but there was no loss in volume when only one of the proteins accumulates within the brain. This suggests that doctors may someday be able to use MRI scans to monitor changes in the brains of AD patients at a microstructural level, before more serious changes begin to take place.
The recognition that symptoms of AD progress from physiological to cognitive can help diagnose those most at risk of developing this disease. These biomarkers might also help with testing the effectiveness of trial medications, and might one day allow physicians to target at-risk individuals with a simply MRI scan rather than a painful lumbar puncture.
The Expanding Role of MRI Scans in AD Diagnosis and Treatment
Non-invasive tests for AD have ramifications that extend well beyond patients themselves, to friends, family, and society at large. The fact is, in addition to being heartbreaking, Alzheimer’s is an incredibly costly disease. Many AD patients require more hospital visits, as well as full-time, long term care. However, accurate and early diagnosis of Alzheimer’s disease could help save $7.9 trillion is medical costs—and relieve some strain on family members and friends.
Thanks to MRI scans and their potential role in spotting Alzheimer's before cognitive symptoms appear, we seem to be edging ever-closer to the ultimate goal of treating AD effectively.
Magnetic resonance imaging (MRI) scans can be crucial pieces of evidence in personal injury lawsuits. The detailed images can convince a jury or judge that an injury occurred as a result of an accident or negligence, rather than aging and genetics.
MRI scans are universally accepted by insurance companies and courts because of their objectivity and superiority to older forms of imaging, like X-ray. Different radiologists may have differing interpretations of the scans, but in general, the results of an MRI scan provide definitive evidence to a judge or jury.
Another great advantage of MRI scans is that they use no radiation, and thus are safer than alternative forms of medical imaging. Instead, MRI scans use powerful magnets to develop highly detailed scans of the body. These powerful magnets require special attention for those with pacemakers or other implanted devices, but scans can still be safely given to most cardiac patients.
Litigation MRI scans are helping everyone from injured motorists to football players with traumatic brain injuries. It's this versatility that makes MRI scans the gold standard for determining medical history.
Unfortunately, MRI scanners at hospitals are expensive and in high-demand.
This may lead the doctor to prescribe rest for your client's injury before signing off on an MRI scan. If you'd like to move your case along, we can help schedule an affordable and timely scan. Precise Imaging has years of experience and accepts cases on lien. Advantages of working with us include:
Fast and easy scheduling - Call Precise Imaging at (800) 558-2223 or schedule an appointment online. We have over 70 locations, many open nights and weekends, to get your scans done quickly and professionally.
A variety of delivery options - Obtain scans on compact discs or other secure media for reliable access. We're experienced in handling potential evidence and same-day reporting is available in many locations.
A range of imaging modalities - Whether you need dual-focus X-ray tubes or an open MRI machine, we've got you covered. For any type of medical imaging, we'll harness our flexibility to get you the best images for your case.
Our facilities are patient-focused - We know that patients who have suffered an injury are under stress and possibly in pain. Our highly trained techs will make sure patients are comfortable and stress-free as they undergo imaging.
Precise Imaging has served more than 150,000 patients throughout California, Nevada, and Arizona. Whether you're an attorney or a patient, we can schedule an appointment at a convenient time and place. Call (800) 558-2223 or make an appointment online.
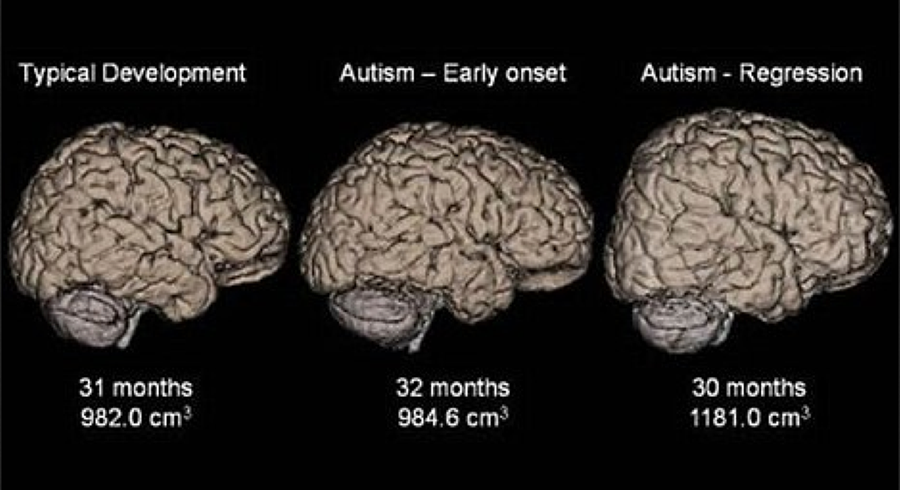
Researchers have observed abnormal neural networks in preschoolers with autism spectrum disorder (ASD) using a specialized magnetic resonance imaging (MRI) technique. The discovery gives hope that MRI scanning may one day allow early diagnosis, intervention, and treatment in ASD.
The study included 21 children with ASD and 21 children with typical development (TD).
It took place over four years in the Chinese PLA Hospital in Beijing. The researchers used a special MRI technique called diffusion-tensor imaging (DTI), which allowed them to observe the location, orientation, and anisotropy of white matter tracts in the children's brains.
Other scientists have used a similar technique to study the brains of patients with Alzheimer disease, multiple sclerosis, epilepsy, and other psychiatric disorders. The approach has led to
an improved understanding of topological organization of the brain network in patients with these disorders.
There were similarly useful results in the study of preschoolers with ASD. The researchers observed alterations of white matter in the children with ASD compared to children with TD. The scientists were able to correlate the alterations in the white matter networks with delays in verbal communication, object use, visual response, body use, and listening response.
The study also observed increased nodal efficiency in children with ASD compared with TD.
That observation agreed with previous studies that had observed this phenomenon in adults on the autism spectrum. The researchers believe this is a reflection of a delayed maturation process in people with ASD.
"Altered brain connectivity may be a key pathophysiological feature of ASD," study co-author Lin Ma told Science Daily. "This altered connectivity is visualized in our findings, thus providing a further step in understanding ASD. The imaging finding of those 'targets' may be a clue for future diagnosis and even for therapeutic intervention in preschool children with ASD."
Medical professionals from around the world weighed in on the study.
"This discovery gives us a more objective diagnostic method by using MRIs to aid us in the diagnosis of children who do have autism, and also gives us a better understanding of the abnormal differences in the brain," psychiatrist Dr. Matthew Lorber told HealthDay Reporter.
Doctors presently diagnose ASD through observing difficulties with social use of communication and interaction in children. A standardized MRI technique that could identify the disorder could give parents and therapists an earlier chance at intervention and treatment.
It's still too early to rely on MRI scans for the diagnosis of autism, but the study's results show that it's possible. The study also provides other researchers with imaging biomarkers that may speed the development of this technology.
Researchers at the Simmons Comprehensive Cancer Center have authored a study detailing a multiparametric magnetic resonance imaging (mpMRI) technique that predicts a malignant type of kidney cancer without performing a biopsy. The results of the method are impressive, but require more refinement to fully take the place of a biopsy.
Doctors frequently find kidney tumors accidentally while conducting CT scans for other reasons.
These scans alone do not yield the necessary information that tells doctors whether they are malignant or benign. Instead, a biopsy is usually performed. These procedures can save lives by correctly identifying the nature of the tumor, but they are also invasive and can cause complications.
“Using mpMRI, multiple types of images can be obtained from the renal mass and each one tells us something about the tissue,” Dr. Ivan Pedrosa, Professor of Radiology and Chief of Magnetic Resonance Imaging told theUT Southwestern Newsroom.
Identifying malignant masses in the kidney is extremely important because treatment is highly effective before the tumor metastasizes. However, once it spreads to other parts of the body, survival rates are low. Clear cell kidney carcinoma is an aggressive subtype of malignant masses that the researchers.
Seven radiologists studied the records of 110 patients with cT1a masses.
These patients had all undergone an MRI as well as a partial or radical nephrectomy. The observing radiologists did not know the final pathology findings, but instead relied on an algorithm to judge whether tumors were metastatic.
The researchers had 78 percent accuracy when rating that the mass was "probably" or "definitely" clear cell kidney carcinoma. When rating that the mass was possibly carcinoma, they had a 95 percent success rate.
The promising results show that biopsies may not be necessary for identifying certain cancers.
Because some patients are reluctant to consent to biopsies, this new technique is potentially lifesaving. As it stands, patients who do not want a biopsy may learn important information if an MRI shows that their kidney mass has a high probability of becoming metastatic. This new information could convince them that the pain of a biopsy is worth going through.
Using these methods to identify clear cell histology is still a work in progress. The doctors at Simmons Comprehensive Cancer Center will have to achieve a higher degree of accuracy in predicting malignant kidney masses for the method to become mainstream.
However, as standardization of imaging protocols and reporting criteria are refined, accurate results should increase. When MRI scans alone are sufficient to identify clear cell kidney carcinoma, doctors will have another powerful tool in the fight against cancer.
Open-Source MRI Dataset from USC Now Available to Researchers
The University of Southern California has released an open-source dataset of anatomical brain images taken from MRIs of stroke victims. The dataset is intended to spur advances in machine learning by providing a large set of manually-traced lesions.
Manually-traced lesions are useful, but labor intensive.
Researchers have attempted to automate lesion segmentation through algorithms. However, this automation is in its primitive stages, and machines cannot yet identify lesions with great accuracy. Thus, manually-traced lesions are still the gold standard, but require a large amount of work from a trained neuroanatomy expert.
USC's dataset attempts to bridge the gap between human tracers and machines. By providing 304 T1-weighted MRIs with lesions segmented by a human, the study's authors hope computer programmers can develop an accurate lesion segmentation algorithm. The dataset is available for download free of charge here.
Strokes are a leading cause of death and disability in the United States.
Mortality rates from strokes have steadily declined worldwide, but around two thirds of stroke survivors suffer long-term disabilities that affect their daily activities. This situation has led scientists to focus on what interventions provide the best outcomes for stroke survivors.
Doctors have opportunities for intervention at both the acute and chronic stages. In the former, intervention can save neural tissue and promote functional recovery. In the latter, rehabilitation can help long-term recovery.
Magnetic resonance imaging can aid doctors in making intervention decisions.
Clinical brain images taken within 24 hours of a stroke help doctors determine whether to administer thrombolytic drugs or perform surgery to save neural tissue. Because clinical scans are taken for almost all stroke victims, there have been great strides in using large-scale datasets of these acute scans for predictive modeling.
Unfortunately, sub-acute and chronic scans are given less and therefore harder to obtain, making predictions at these levels less advanced. That's one thing the study's co-author Sook-Lei Liew would like to change.
“The goal of ATLAS is to generate a dataset that machine learning and computer scientists could use to develop better automated algorithms to identify the lesions,” Liew told Health Data Management.
Machine learning requires large, accurate datasets to train and to test.
Liew hopes that computers will eventually be able to identify biomarkers in stroke patients, making it easier to prescribe the appropriate rehabilitation therapy and treatment. Her next step is to create a separate dataset used to test the algorithms developed using the current dataset.
“In machine learning, you always need a training dataset and a testing dataset." Liew noted. “Even if people aren’t interested in stroke, it’s also an interesting dataset to train any sort of computer vision algorithm because it’s a challenging problem.”
References:
Slabodkin, G. USC Releases MRI Stroke Dataset To Spur AI Research. Health Data Management. Available here. Accessed February 22, 2018.
Liew, S et al. A Large, Open Source Dataset of Stroke Anatomical Brain Images and Manual Lesion Segmentations. Scientific Data. February 20;(5):180011. doi:10.1038/sdata.2018.11
Accessed February 22, 2018.
Feigin, VL et al. Global and regional Burden of Stroke During 1990-2010: Findings From the Global Burden of Disease study 2010. The Lancet. January 2014;(383)9913:245-255. doi:10.1016/S0140-6736(13)61953-4 Accessed February 22, 2018.
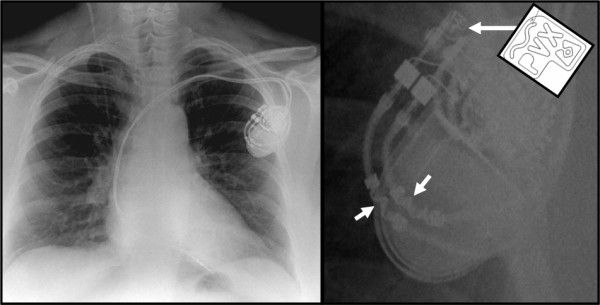
Patients with pacemakers and implantable cardioverter-defibrillators (ICDs) may safely receive magnetic resonance imaging (MRI) testing according to a study from the New England Journal of Medicine. Currently, implanted devices must meet the Food and Drug Administration's criteria to be considered MRI-conditional. The pacemakers and ICDs that do not meet these requirements are considered legacy devices, and the federal government considers them unsafe for MRI scans. However, the new study proves that, with adherence to protocols, patients with legacy devices can safely receive MRI scans.
The study followed over 1500 patients with implanted devices.
The prospective, nonrandomized study followed 875 patients with pacemakers and 634 with ICDs. All patients had implanted devices that were considered legacy devices — that is, they did not meet the requirements of the Centers for Medicare & Medicaid Services (CMS). Researchers from the University of Pennsylvania performed MRIs on the patients only when it was deemed clinically necessary.
The scans were done under strict protocols with physicians on hand to monitor patients. Tachyarrhythmia functions were disabled on the machines and pacing modes were appropriately adjusted on the devices.
“We found MRI examinations to be safe in the setting of legacy cardiac pacemakers or ICD systems, when using a safety protocol,” lead study author and University of Pennsylvania professor Saman Nazarian toldCardiovascular Business. “The scans were safely performed even when performing thoracic or cardiac MRI and with patients that were dependent on cardiac pacing for every heartbeat.”
A previous study from MagnaSafe found similar results for non-thoracic scans.
The MagnaSafe Registry is a multi-center study attempting to determine how safe MRIs are for patients with pacemakers and ICDs. They published findings several years ago that upended the traditional view that MRIs were too dangerous for patients with legacy devices. With similar results to Nazarian's study, MagnaSafe found that there were almost no clinically relevant problems caused by the scan.
This is hugely important because many people with legacy implants are denied MRI scans by Medicare and Medicaid. While doctors may then order computed tomography (CT) scans, MRIs are better at diagnosing certain diseases, particularly in the brain and spinal cord. Nazarian said that if a patient with a legacy device needs an MRI, they should contact a medical center that can safely conduct the scan.
“Many centers across the U.S. are capable of performing safe imaging despite your device,” Nazarian said to Cardiovascular Business. “MRI can be instrumental in providing the right data for appropriate treatment planning in the setting of many neurologic, cardiac and musculoskeletal disorders as well as malignancies.”
The results from the two studies offer compelling evidence that MR technology is safe for those with implanted legacy devices.
According to Robert Russo, a doctor in the MagnaSafe study, more than half of patients with implanted devices will eventually need an MRI. Replacement with an MRI-conditional device is not an option, as the complication risks are too high. Therefore, it's important to determine the safety of MRI scanning for patients with these legacy devices.
The above studies show how MRIs pose minimal risks while bestowing life-saving advantages for those who need scans. The FDA and CMS have not changed their regulations in light of the findings, but the evidence is mounting that they should consider doing so.
Nazarian S et. al. Safety of Magnetic Resonance Imaging in Patients with Cardiac Devices. The New England Journal of Medicine. December 2017;377:2555-2564. doi:10.1056/NEJMoa1604267
Personal injury attorneys have relied on MRI scans to bolster their clients' claims for years, but the role of this crucial technology may soon grow dramatically. As a diagnostic imaging modality, MRI is ideal for recording soft tissue injuries, including disc protrusions and herniations and muscle tears. But even perfect documentation of these injuries doesn't necessarily prove a devastating type of affliction that's all too common, and often difficult to demonstrate: chronic pain.
Pain is a subjective sensation. One person's agony might be another's slight discomfort, and defense attorneys have a history of leaning on this subjectivity to reduce damages. Meanwhile, though, patients' lives can be destroyed; ravaged by pain, they might not be able to work, or even perform daily tasks of living. A fair settlement might be the only thing that stands between them and utter destitution.
But how can an MRI scan document pain? Neuroscientists say they're right on the verge of an answer.
Using MRI Technology to Track Pain's Pathways in the Brain
A specialized type of MRI scan, functional magnetic resonance imaging, or fMRI, measures blood flow within the brain. When a certain region of the brain activates, cerebral blood flow in that area increases. The fMRI tracks these changes.
Brain mapping allows neuroscientists to associated certain areas of the human brain with general functional experiences within the thinker — including, perhaps, the thinker's experience of pain. If an attorney could demonstrate that a client's brain activity is consistent with chronic pain, that could be enough to sway the judge. However, we're not quite ready to break out the fMRI scans in tomorrow's personal injury case.
Hurdles in the Use of fMRI Scans for Personal Injury Cases
Neuroscientists are still debating the reliability of fMRI to demonstrate chronic pain. Most of the studies involving pain and brain mapping have been conducted on acute pain, not the chronic variety. Some scientists argue that patients could "cheat" the scan, imagining a greater-than-baseline intensity of pain.
The science behind demonstrating pain with fMRI scans isn't quite up to courtroom standards yet, but it's close, and it's getting closer. With every new study on the subject, fMRI technology inches toward a future in which pain is as visible as a broken arm in an X-ray.
Meanwhile, standard MRI scans continue to be an important element in many personal injury cases. This technology has changed the way personal injury law functions, and it appears it will continue to do so in a broader range of cases soon.
Radiologists and referring physicians need dependable, clear communication to collaborate on accurate diagnoses for their patients. When that communication is lacking, the risk of errors can quickly compound.
Annette Johnson, MD, MS, describes a particularly worrisome case on the Agency for Healthcare Research and Quality website. This is an example of what can go wrong when physicians and radiologists don't have quick, easy-to-use access to one another.
Radiology Report Transmission Errors: An Alarming Story
A 62-year-old man was admitted to the hospital with swelling in his abdomen and legs, Johnson reports. His right leg was slightly more swollen than the left, and the attending physician was concerned that he might have a deep vein thrombosis (DVT). The physician ordered an ultrasound to check for evidence of a blood clot.
The imaging procedure didn't show any signs of DVT. The radiologist called the primary care team and told them this verbally after dictating the report, so the team continued to treat the man with the understanding that he did not have a DVT. All was well up to this point.
The problem occurred when the night team rotated in. As the radiologist verbally dictated the report, it turns out, the dictation system clicked just as it recorded the words "no DVT is seen" — obscuring the word "no." As a result, the hospital's voice recognition software recorded the phrase "DVT is seen." That's the statement that made it into the truncated radiology report, which the night resident read when beginning the shift.
This confusion eventually led to two unnecessary surgeries: One to place a filter in a blood vessel leading to the lung, to block the (nonexistent) blood clot; and the other to remove the filter after someone finally tracked down the reporting radiologist and learned about the mistake. The good news is that there were no complications, and the patient emerged from the surgeries no worse for wear.
Improving Communication Between Radiologists and Referring Physicians
So where did the care team go wrong in this case? Let's break the issues down into two categories: technology and procedure.
There were two clear technology issues in this case: First, a microphone that clicks when activated, and second, the voice recording software's inability to understand the word "no" beneath the click.
But the case also illustrates the simplest way around reporting errors. Remember that when the patient was first admitted, the reporting radiologist spoke directly to the primary care team. That sort of one-on-one interaction is ideal.
At Precise Imaging, we offer a physician's web portal that allows real-time sharing, analysis, and annotation of diagnostic images. This provides yet another way for physicians and radiologists to collaborate directly, no matter where they are.
As for procedural issues, Johnson points out that dictation using VRS is more error-prone than using human transcriptionists. Of course, her report dates back to 2011, and voice recognition systems have improved since her estimation.
The team also missed the opportunity to provide all physicians involved in the patient's care with access to more information — while the truncated radiology report might have read "DVT is seen," with access to images, annotations, and detailed analysis, the night resident might not have proceeded under the assumption that a blood clot was present. Again, comprehensive image-sharing web portals for physicians offer greater communication between radiologists and physicians.
Physician web portals aren't the only innovation that can improve information-sharing between all members of a medical care team. You also need experienced, board-certified radiologists who work onsite in the U.S. to read diagnostic images, such as those at Precise Imaging.
All of our radiologists are devoted to patient care, and that means excellent communication with doctors, every time. Radiologists and referring physicians can work together to improve patient outcomes — but only if they commit to quality communication.